India Fieldwork Experiences
Shatabdi Das Bio
Shatabdi Das is an MPH student in the Division of Epidemiology and Biostatistics. Shatabdi traveled to Hyderabad, India under the preceptorship of Dr. Mark Dworkin from the UIC School of Public Health, and Sabitha Rajesh and Dr. Vijay Yeldandi from SHARE India, the project aims to assess the feasibility and acceptability of a mobile phone-based health intervention for educating about HIV and supporting antiretroviral therapy (ART) adherence among low socioeconomic and low health literacy HIV-positive individuals in Hyderabad, India. Shatabdi will conduct interviews in Hindi over eight weeks, to evaluate knowledge of HIV/AIDS, ART adherence, and factors such as depression, social support, and health literacy. Additionally, Shatabdi will conduct a comparative literature review of existing mobile phone app-based health interventions for ART adherence and monitoring in HIV patients across various countries.
Mark Dworkin Bio

Dr. Mark Dworkin is a board-certified Infectious Diseases physician with a Master’s Degree in Public Health and Tropical Medicine who was trained in the CDC’s Epidemic Intelligence Service program. As a professor and Associate Director of Epidemiology in the Division of Epidemiology and Biostatistics at the University of Illinois at Chicago School of Public Health. During December 2023, Dr. Dworkin traveled to Hyderabad, India with two UIC PhD Students to work with collaborators, SHARE India and Chaithanya Mahila Mandali (CMM), in preparation for a research study using an mHealth intervention among people living with HIV (PLWH).
Casey Luc Bio

Casey Luc, MPH is a PhD candidate in the Division of Epidemiology and Biostatistics. Casey traveled to Hyderabad, India with Dr. Mark Dworkin to work with collaborators, SHARE India, in preparation for a research study using an mHealth intervention among people living with HIV (PLWH). While in Hyderabad, Casey visited local non-governmental organizations (NGOs) that support the LGBTQI+ community. With the help of the NGOs, Casey spoke with a small number of MSM living with HIV to learn about the experience of being a gay/bisexual/same-gender-loving man in India as well as how COVID-19 impacted their ability to access HIV care. These conversations provided important context for the soon-to-be mHealth intervention. Casey is grateful to the Passaro family and Wayne Wiebel for supporting this life-changing opportunity.
Kara Nitti Bio

Kara Nitti, MPH is a PhD candidate in the Division of Epidemiology and Biostatistics. Kara traveled to Hyderabad, India with Dr. Mark Dworkin to work with collaborators, SHARE India, in preparation for a research study using an mHealth intervention among people living with HIV (PLWH).
Kara Nitti's global health research and practice in Hyderabad
Kara Nitti
Kara Blog

I was fortunate enough to travel to Hyderabad, India with my advisor, Dr. Mark Dworkin, and another PhD candidate, Casey Luc. In Hyderabad, I spent a week with UIC staff and our collaborators, SHARE India, in preparation for a research study using an mHealth intervention among people living with HIV (PLWH). While there, I also gained a holistic view of health care and access for PLWH, as we visited various community hospitals and non-profit organizations conducting outreach to target populations in India. Read more about my field work and global health experience below!
December 6, 2022

We met with SHARE India staff and clinical staff at a government funded community hospital serving predominantly acute care, surgical, and labor and delivery patients. We were able to tour the hospital, learn about future improvements to equipment and patient capacity, and review SHARE India strategies for infection prevention protocol improvement. I was particularly interested in the clinical flow for HIV/STI testing, and despite being over patient capacity, was impressed with the continuity and linkage to care for positive cases to HIV/STI counselors.
We met with a coordinator from SHARE India, Sabitha Gandham, and conducted a mock interview in preparation for the upcoming study. We provided feedback on qualitative interviewing techniques and reviewed the mHealth intervention we created, an Avatar that speaks the local language and provides education. Sabitha speaks three languages, including Hindi, the national language of India, Telugu, a regional language spoken in Hyderabad, and English. She will be conducting the interviews in Telugu.
Dec 7 Blog
We visited an ART center to learn about how people living in India get tested for HIV and prescribed antiretroviral therapy if they test positive. ART in India is government funded and free of charge to all of those who need it. We learned about their central reporting processes for new HIV cases and additional information, like viral load and CD4 count over time. While there are ART centers in each district, the largest issue is still accessibility and lack of transportation as patients are required to pick their medicine up in person and may travel long distances, making it a challenge for those who don’t want to reveal their status to others.
We met with a local community organization, HOPES, who do outreach work to PLWH and provide them with social services, particularly men who have sex with men (MSM) and female sex workers (FSW). We conducted an informal qualitative interview of an MSM LWH to understand his unique perspective of living in India as an MSM LWH during the pandemic. In general, he felt isolated and depressed during the pandemic due to lack of social support but relied heavily upon their network of MSM, as opposed to family or other friends.
Dec 8
We conducted another mock interview with the SHARE India coordinator who will be administering the interviews. We provided feedback on qualitative interviewing and reviewed the intervention again. We had a team dinner, consisting of local Indian dishes, such as tandoori masala, chicken biryani, palak paneer, and chapati. While Hyderabad is known for chicken biryani, I really enjoyed eating all of the vegetable dishes they had to offer as well.
Dec 9

One of my favorite activities while in Hyderabad was when we visited the non-profit organization, Chaithanya Mahila Mandali (CMM), which provides shelter and social services for daughters of female sex workers in order to prevent second generation forced sexual slavery. The organization also provides vocational training, education on reproductive health and rights, and ultimately combats human trafficking. We met 43 girls and boys who live on-site at the CMM facilities and learned about their day-to-day lives, education, and toured where they live. We also met with the founder, who shared his long-term visions for the organization. We learned about the challenges the founder faced to secure the land and build the current estate.
Children at Chaithanya Mahila Mandali

Despite these challenges, it was inspiring to see the safe space the organization has provided for these destitute children. After this visit, I felt compelled to raise funds that will go directly toward supporting operational costs and completing the facilities, such as providing a safe outdoor space for the children to play. To read more about the fundraising effort, please visit my LinkedIn page.
Continue Dec 9

Young girl jumping rope at Chaithanya Mahila Mandali
Dec 10

We visited Sivananda Rehabilitation Home for Leprosy, Tuberculosis, and HIV. We met with the clinical team and learned about surgeries they perform there to improve deformities caused by Hansen’s Disease, splints that they make on-site for patients to use, and rehabilitation methods, such as stimulation and exercises used before and after surgery. While there, we also met with staff from SHARE India and discussed current tuberculosis focused projects, particularly latent tuberculosis, and CDC-funded projects. In the afternoon, we visited Charminar, a 16th century mosque and market. From silks to samosas, the market had many local offerings.
Dec 10 Continued

Vendor at Chaminar
Dec 10 Cont
Locals at Chaminar
Dec 10 Final

My time in Hyderabad with our collaborators, SHARE India, was remarkable. As an infectious disease epidemiologist with a focus on HIV/STIs, I am extremely appreciative I was afforded the opportunity to travel to Hyderabad and learn about health care in India for PLWH and the barriers they face. If you have an interest in HIV among FSWs in India, check out my abstract “Factors associated with antiretroviral adherence among south Indian female sex workers living with HIV” here. Thank you again to the Passaro family for supporting my passion for global health and infectious disease, my advisor Dr. Mark Dworkin, for connecting me with our collaborators in India, and SHARE India for their expertise and hospitality. Until next time!
Mayuko Takamiya Bio

Mayuko Takamiya, MPH in Epidemiology ’18, traveled to Hyperabad, India to collaborate with SHARE India and Chaithanya Mahila Mandali to study food insecurity and medication adherence among female sex workers with HIV. Check out her blog posts from the trip below.
Mayuko Takamiya
Mayuko's Blog Post
My six week stay in India finally came to an end. In conclusion, we are still waiting for the IRB approval from the local research institute. Each week, I had hoped to hear some good news but the first review of the protocol still hasn’t happened after almost two months. I heard they don’t have a fixed monthly schedule of committee meetings like many research institutes in the U.S. and therefore, a date of the committee meeting for protocol reviews completely depends on schedule and availability of the committee director. This kind of turn of events just happens when it happens.
But I am still glad that I came all the way to India because even though I could not be a part of the actual data collection process, there was still a lot that I can do for the research. Such as piloting questionnaires with peer educators, meeting with local researchers in person and making sure in detail that we have a mutual understanding on all the research steps and translations to avoid instrumental errors, doing some field inquiring surveys on nutritional support for female sex workers living with HIV/AIDS, hearing real voices from peer educators and outreach workers about food insecurity and medical adherence, learning about the host NGO and gaining deeper insights into background information and other related issues (i.e sex trafficking, prejudice toward female sex workers, lack of support for children whose mother is a sex worker, urban slums, children’s education in remote countryside etc.).
Moreover, I was blessed with all the serendipitous, priceless experiences and encounters with wonderful people and unforgettable sceneries. Particularly living with 45 children and getting to know each one of them was the most delightful part of my stay. On the last day, I made 50 papaya, pineapple & yogurt ice popsicles with help from some girls for the children and people at the local NGO to show gratitude. I forgot to take a photo of it because we had to deliver the ice popsicles from my apartment to the Children’s Home before they melted!
Returning to the U.S. does not mean my job is finished. After obtaining the IRB approval from the local research institute, they will start the research and we will work on data analysis to see what we can learn from the pool of data. For an epidemiology student like myself, that will be a great learning opportunity to practice and apply epidemiological and biostatistical skills in real life settings. Thank you for reading my blog and your support. I hope you enjoyed!
.

*The contents of this blog do not represent any position of the School of Public Health but are mine personally. All the photos used are taken by me.
AUGUST 3, 2017; URBAN SLUM
In my final week in India, I had a unique opportunity to visit a slum area in Hyderabad with my host organization, Chaithanya Mahila Mandali (CMM). Needless to say, this day trip left a powerful impact on me and I am very thankful for CMM to let me tag along with their visit to the slum area. It was a part of CMM’s newly launched program to support children in urban slum areas and we visited a school to provide educational supplies like notebooks, pencils, and erasers.
The neighborhood we visited is called Green Park Colony (although the name sounds ironic for a slum) and located in northwestern suburbs of Hyderabad. We drove for about forty minutes and got lost in the middle of a quiet, middle-income neighborhood for a while. After asking a few locals for directions, we managed to find Green Park Colony. Identical collective apartments painting in light pink stood side by side and radiated vibrant lived-in feel. People from CMM explained to me that these collective apartments and school were built recently by the government for low-income families. At first, I thought everything looks more developed on the surface than I imagined from pictures of slums in other cities in India. These six story housings did not look too different from any other average apartments and there seemed to be electricity-installed, which I realized, later on, was just only the case for this restricted part of the slum.
Alley

Alley in India.
.

After handing over educational supplies to children at school, we strolled around the other side of the neighborhood. In fact, the core part of the slum, consisting of hundreds of shacks, was revealed in front of us after a few blocks of the collective apartments. It was as if the apartments separate between the slum and non-slum neighborhood like an insulating wall. Most of the shacks were built from tin sheets and some bricks. No water pipe system was installed. People buy water from a water truck and keep it in blue tanks outside the shacks. The water is used for all the necessary daily activities like drinking, cooking, and bathing. Some shacks were built below the ground level, which makes it disastrous in rainy seasons because all the sewerage ridden water soaks the living area.
People from CMM told me that most of the residents are migrants from rural areas and jungles and also roughly 50-60 percent of female sex workers they support come from this neighborhood. I asked how these people are making a living and they explained that people (both men and women) stand on a specific busy street nearby and wait for daily employment including construction labor, painting walls, and other cheap labor work. Furthermore, women are often a target for unpaid, forced sex work. Women get hired to work at construction sites or else during the daytimes and, as night work, they are forced by a construction manager/pimp to sleep with men. They get paid for construction work (400 rupees per day) and that’s all after working day and night. However, regardless of the unpaid sex work, they still line up for this kind of daily employment because that is the only way to make a living around this area for illiterate slum women.
Drying Clothers

Women drying clothes.
.

Although garbage was everywhere and a pungent smell of everything pervaded the air, the everyday-life sceneries of the people were laid back, chill and somewhat peaceful. Some women were sitting on the ground and cooking. Other women were hand-washing clothes. Next, to bleating goats, children were running and playing. Some men were sitting on a chair outside.
The living conditions look far different from ones we are familiar with but there are people who spend most of their life there and to them, this is the reality of everyday life. As a complete outsider, I wanted to make sure everything I speak and do is respectful to the people and my visit does not disturb their daily life sceneries as much as possible. Particularly, I was sensitive about photography because I did not want anyone to feel like they are an object that a random outsider can come and take a snap out of only because they are poor. I wanted to capture over one million people’s reality as a graphic form and bring it back home so that it can always remind me of what I saw with the same vivid sensation as the day I visited. When I wanted to take some photos, I asked them for permission and took it only when they said they are comfortable with it.
The urban slum presumably faces all the same problems as other slums; a lack of basic infrastructure (i.e water pipe system), safe housing and decent jobs. These things need to be fixed and improved and, the Indian government is under its way of doing so as seen from the newly built apartments and school. But I also witnessed that the slum isn’t just about abject poverty and hardship. The slum is an epitome of vitality and, most of all is the home for its residents. The slum visit marked the highlight of my final week in India and I started packing after returning to my apartment.
*The contents of this blog do not represent any position of the School of Public Health but are mine personally. All the photos used are taken by me.
Mayuko's Blog Post
As my return date is fast approaching, I decided to make a visit to some local markets that I wanted to see. I always like to visit local markets in any country I go because I feel I can sneak-peak the everyday life of the locals. I am curious to know what the locals shop every day to eat, dress, utilize and decorate. Through such experiences, I gain insights into the lifestyle, beliefs, and values that consist of the everyday life of the locals.
The first market is Gudimalkapur Flower Market in the Eastern suburb of Hyderabad. The flower market opens every day from 5:30am and sells out most of the flowers by 10:30am. Every morning, wholesalers bring in bags full of colorful fresh flowers like Marigolds, Jasmines, and roses, which have spiritual meanings in Hindu. The locals come to the flower market and buy bagful flowers for their home. Flowers are essential for Hindu people. By decorating temples, cows and sometimes themselves with flowers, they express their faith in the gods and goddesses. The market was vibrant in colors and filled with the mixed aroma of different flowers. Religious faith is a fundamental part of people’s lives and I see flowers anywhere religious in this country.
Local Market

Clothing in a local market.
.

Next, I visited Monda Market for spices. Needless to say, spices are essential ingredients in various aspects of people’s lives in India. There are numerous spices– such as turmeric, red chili, pepper, cinnamon, mustard seeds and cardamom– that are used for Indian cuisine, traditional medicine, religious purposes and even fashion in India. People believe each spice has a different health benefit according to Ayurvedic beliefs and people naturally incorporate the use of spices in daily diet and medicine. Ayurveda is traditional Indian medicine with a history of thousands of years. Spices are often used with religious meanings too, such as bindi. Bindi is a trademark of Hindu and Jain people on their forehead as the third eye and is pigmented with a mixture of turmeric and limestone. On a wedding, people color their feet in yellow with the haldi paste made from turmeric, rose water and sandalwood powder.
Market 2

Spices in a market.
.
Besides spices and flowers, local markets are filled with fruits, cheap bangles, colorful silk textiles used for scarves and sarees, and anything necessary in the everyday life of the locals. On the other hand, you see a cow, goat, hen and stray dog casually strolling around and plastic bags, rotten fruits and vegetables thrown out on the side. So many things are going on and two eyes are hardly enough to capture everything happening at a local market.
The west side of Hyderabad is so called the new district where you see all the high technology corporation offices, newly built high-rise condos, and affluent people and foreigners enjoying the modern westernized lifestyle. I didn’t have a chance to pay a visit to the new district this time but it must be where you would witness the new face of India as the fast-growing tech power in the world. However, even though some parts of the country have been transformed under the name of economic growth, I bet India of ordinary locals jammed with the filthy and the beautiful altogether has not changed so much since the old days, and which can still be seen in places like local markets. And that’s why I wanted to visit them.
*The contents of this blog do not represent any position of the School of Public Health but are mine personally. All the photos used are taken by me.
Mayuko's Blog Post

One of the historical sites in Hyderabad that I wanted to visit is the Chowmahalla Palace in the Old City area. As a world history lover, I was fascinated to learn the city is so rich in history. This place was a must-go before my return date.
On my final weekend in India, I decided to visit this place. The opulent palace had been used as an official residence of the Nizams (kings) during the dynasty of the seven Nizams (also called Hyderabad State) from the eighteenth to twentieth century. Following the decline of the Mughal power in the early 1700s, the seven successive Nizams had ruled the central part of South India until the independence of India from the British colonization in 1948. The rule of the Nizams had continued even after the British victory in the Second Anglo-Maratha War in 1805 by becoming under the protection of the British East India Company. The Nizams built numerous hospitals, universities and schools and set up infrastructure in Hyderabad and surrounding regions. The Hyderabad State became the richest region in India by the early twentieth century.
I could see from the palace how Hyderabad had been actively interacting with foreign countries during the times of the seven Nizams. As the palace was built resembling a palace in then-Persia (current Iran), Persian influence is vivid in the palace structure and upholsteries, which interweaves the unique Indo-Persian style. From the display of beautiful gifts from all over the world, I learned that the Nizams had established active diplomatic relationships with Persia, the British Empire, China, Japan, Germany and many other countries.
.

Inside Chowmahalla Palace
.

To me, the palace appeared to symbolize the harmonious amalgamation of history and the present, and of Indian and neighboring culture (particularly Persian-Islam culture) in Hyderabad. More intriguingly, I feel such culture has blended in people’s life even today. What Hyderabad is today is shaped by the legacy of its unique history, which can be observed in the language, customs, cuisine, architecture, religions and social systems of Hyderabad.
Mayuko's Blog Post

Although we might imagine Hindu as the national religion, India is in fact a very multi-religious country. When you are on a street in India, it is almost impossible not to witness a sign, decoration, praying facility or people’s attire that is related to different religions and, somehow all of them harmoniously blend in together (or at least they seem to from an outsider’s eyes). In Hyderabad, there are six religions that I have been seeing on streets so far; Hindu, Islam, Jainism, Christianity, Zoroasterism, and Sikh. I know religion is considered as one of the sensitive topics like politics to discuss. But for me, who grew up in an environment where religion did not play a huge role, learning about different religions and witnessing how they are so fundamental to people’s lives in India is intriguing and even fascinating. It got me thinking many times what religion is all about.
The most major religions in Hyderabad
The most major religions in Hyderabad are Hindu and Islam. Particularly for Hindu, taking pictures of religious objects and its people yield the most India-like, picturesque images. It is simply because everything is full of vibrant, awaking colors. At Hindu temples which you can find everywhere in the city, the gods and goddess are painted with multi-colors. At flower markets, wholesalers hand-craft and sell religious decorations with Jasmine flowers, Marigold flowers, roses, lotus, and hibiscus. At any local market, you can find mountains of spices and bindi powder (bindi is a red or orange mark on the forehead of Hindu-people).
Hindu population in Hyderabad is about 60 percent. The second most popular religion is Islam which consists of about 30 percent. With the historical legacy of the dynasty of the seven Nizams that had ruled some parts of current India and Pakistan, particularly the Old City area of Hyderabad is Muslim-dominated and Urdu is commonly spoken and written there. Urdu is a language widely spoken by Hyderabadi Muslims and has received strong influences from Arabic and Persian. It is also an official language of Pakistan, India’s neighboring country. Because of the ongoing dispute between India and Pakistan over Kashmir, I was surprised at first to see the Pakistani official language is everywhere in Hyderabad and to find a franchised bakery chain named Karachi Bakery being popular among the locals (Karachi is one of biggest cities in Pakistan). Historically speaking, the official religion of the dynasty of the seven Nizams in Hyderabad had been Islam and the city has been under strong influences of Islamic culture. I thought, in Hyderabad, the Islamic influences might be one of the factors that help to alleviate the negative public sentiment of locals toward Pakistanis.
.

The other religions
There are also other religions like Jainism, Christianity, Zoroasterism, and Sikh. I have seen a few Jain temples, which at first I thought are Hindu temples until I learned the symbol of Jainism. Jainism believe in ultimate harmlessness and possession-less and are known for extreme veganism. Christianity also exists mainly in the sister city of Hyderabad, Secunderabad. Secunderabad is a relatively new area in Indian history which is probably why Christianity settled there as a newly introduced religion. Sikh is also a popular religion in India but is rather a minor one in Hyderabad because I hardly saw anyone with a Sikh turban.
Like Islam, Zoroasterism originated from ancient Persia and is one of the legacies from the dynasty of the seven Nizams. Zoroastrians believe that fire, water, earth, and air are sacred and worship fire. My first encounter with Zoroasterism in Hyderabad was the Tower of Silence near my apartment. I noticed on the Google Map that there is a site called Tower of Silence within the radius of 1.5km from my apartment and I vaguely wondered what it was. A few weeks later, I was walking back from the visit to the Gandhi Hospital and realized I was walking along the Tower of Silence. The site was surrounded by a stone wall and looked forestry inside. It was quiet and I could not see much from outside the wall. I learned to my surprise, that the Tower of Silence is a tower used for disposal of corpses by Zoroastrians based on a belief that the sacred earth should not be polluted by the dead. The corpses are exposed to the sun and scavenging birds on a roof of the tower. In other cities and countries in the Central and South Asia, this Zoroastrian way of corpse disposals has been banned today due to the decreases of vultures in urban areas and spread of infectious diseases. However, this practice is not banned in Hyderabad yet.
Coexistence of Multi-religions
Having five or six different religions, how does the society maintain its harmony? There is one photo of the unforgettable wall painting that I saw at an elementary school in the rural area. Next to an alphabet chart, a title “Oh Lord Grant Me” and the following were written;
“ The heart of Buddha The Brain of Shankara The Body of Mohammed The Purity of Zoroaster The Forgiveness of Jesus Christ The Fearlessness of Vivekananda The Divine Experience of Ramathirtha The Non-violence of Mahatma Gandhi “
In a multi-religious country like India, I guess acknowledgment and appreciation of different religions are key for unifying the country as one. Of course, it is not an easy thing to accomplish. To me, this painting at the school seems to symbolize India’s effort and wish to maintain the harmonious coexistence of multiple religions.
Mayuko's Blog Post

Previously I had a chance to tag along with the host organization, Chaithanya Mahila Mandali (CMM)’s day trip to schools in rural areas of Hyderabad. Two weeks later, we had a second visit to schools in different parts of rural Hyderabad that we couldn’t visit previously to donate educational supplies. The schools that CMM has provided free educational supplies for are all government schools (public schools).
As a side note, tuition for public schools in India is around $300 while $2200 for private schools. The tuition for Indian private schools sounds very reasonable compared to American private schools but you can imagine how it is not the case for the ordinary locals* when private schools cost seven times more than public schools. (*Affluent Indians often send their children to England, the United States, Canada or Australia for education and can afford extraordinarily expensive tuition for international students. On the other hand, there are the poor who are illiterate with no proper means to make a living in India. The social inequality in India is very large, so the phrase “ordinary locals” might be too vague to capture who is being referred to.)
Why do I write about the rural school visit that I wrote about in a similar post already? Well, these schools on the second visit left some strong impressions on me for a variety of reasons. The key words are “a boiled egg twice a week,” “stone cutting” and “local newspaper.”
A Boiled Egg Twice a Week
When we arrived at the first school, it was lunch time where children were lining up for food at the playground. Being distracted by the sudden visitors with one foreigner (me), the children were lively enjoying their lunch. The children were energetic and very curious about me. One kid asked me what my name is. Then, in the next moment, ten more kids asked as well. When one kid asked me to shake hands, ten more kids asked to shake hands. It was hilarious and amusing to get “question attacked” from the children. The lunch of the day was steamed white rice and dal curry (legume curry). The dal curry seemed like every other dal curry I’ve seen in India but the project manager from CMM explained to me that it is diluted with water to increase the volume. While lunch is provided for free by the government because it is a government school, a nutritional deficiency was one of the concerning issues at the school. A boiled egg twice a week is the only major source of protein provided for lunch (except the legume in the water-diluted dal curry). Some girls had patches of lighter pigment on the skin due to nutritional deficiency, the headmaster explained.
.

Stone Cutting
The second school was more remote from the city and the building was much smaller. Around this area, stone extracting and cutting are the main industry besides agriculture. When I learned this, the Oscar winning film, Lion (2016) occurred to me in my head. If you have seen the film, you might remember Saroo’s mother carried stones for money at a quarry. From a car window, I saw gigantic machinery outside on empty fields, which I assume are used to extract and cut stones. I learned that many of the children at this school work at a stone-cutting quarry after school. Seeing the gigantic metal machinery outside, it gave me a chill to think about how dangerous the work would be especially for children.
Faced with the reality of nutritional deficiency and child labor at quarries at the two different schools, I just felt bewildered and helpless at this contrast with children’s lively laughs and smiles. Although I knew these things are still happening somewhere in the world, witnessing them with own eyes leaves a much stronger and powerful impression.
Local Newspaper
After a week from the rural school visit, the project manager at CMM showed me a local newspaper article that mentioned about our visit to the rural schools, which I happened to be in one of the group photos we took. Of course, I took a screenshot of the article!
.

Newspaper
Mayuko's Blog Post
In this post, I would like to talk more about our research and the planning process prior to my departure to India. Back on September 16th, I had a talk with Dr. Mark Dworkin, the Infectious Disease Epidemiology professor at UIC and my academic advisor. During the talk, he mentioned the medical adherence research in India that he conducted in the past and a new research proposal he had in mind. As my interest lies in pharmaceutical research in the context of global health, his research topic sounded intriguing. With one more second year MPH student, Christina, we started to plan the research protocol about the medical adherence among female sex workers living with HIV.
Background and Hypothesis postulation [October-November]
To further educate ourselves and prepare the research in depth, we started literature reviews on adherence to HIV medicine among female sex workers in India. Identifying what we know so far from past literature and what we don’t yet know allowed us to narrow down what hypothesis should be postulated, what research type is appropriate and what we want to know out of this research.
1. Location: India
India is home to 2.1 million people living with HIV/AIDS and is ranked as the country with the third highest number of people living with HIV in the world, despite the free provision of antiretroviral therapy (ART) by the Indian government.
2. Problem: Non-medical adherence to ART
Suboptimal levels of medical adherence (adhering to medicine as prescribed) lead to inadequate viral suppression, a progression of a disease, lower quality of life and risks of co-morbidities. From the public health perspective, medical non-adherence poses an immense challenge that increases the burden of HIV/AIDS not only on an individual but also on a population-scale. Low levels of medication adherence among HIV-infected individuals can contribute to increased HIV transmission due to lack of viral suppression and development of resistant virus.
3. Potential key factor: Food insecurity
Food insecurity refers to a lack of social, physical and economic access to sufficient, safe and nutritious food to meet dietary needs. Typically, hunger and malnutrition are the direct consequences of food insecurity and is ultimately experienced by individuals suffering from poverty. Some past research results suggest that food insecurity can interfere with an ability to adhere to ART because some people may not take ART to avoid an unwanted side effect of ART on an empty stomach.
4. Target population: female sex workers
Numerous past literature supports that female sex workers are one of the priority groups in HIV/AIDS control in India. Furthermore, Dr. Dworkin’s previous research in India has shown that female sex workers have the lower rate of adherence to antiretroviral therapy (ART) than other subgroups.
To the best of our knowledge, there is no published research investigating on food insecurity and ART adherence among sex workers in India. Therefore, our hypothesis was postulated as “food insecurity and adherence to antiretroviral therapy (ART) are associated among female sex workers living with HIV.”
Documents Preparation [December – April]
By December, we moved onto creating documents like a questionnaire, informed consent, protocol and other necessary documents. We contacted each other via emails regularly and met up for discussions on drafting the documents almost weekly during the spring semester. The research instruments must be written in appropriate use of language that conveys accurately what we intend to convey, that FSWs can understand and that is culturally sensitive about asking private questions like income, sexual work, HIV status etc. In early April, we were ready to proceed with the IRB process.
Institutional Review Board (IRB) process [April-July]
IRB review is required for all research with human subjects to assure they are performed in an ethical manner to human subjects. Completing a 30-page IRB application and 4 appendices, we submitted all of the research documents to the OPRS Live website for the IRB review in the early April. After the first expedited review, it was decided that we are required to submit a full review to obtain the IRB approval for this research because the research subjects are considered socially vulnerable instead of healthy normal subjects. Modifying and clarifying contents of the IRB documents, according to their 3-page-long lists of feedbacks, we submitted the modified documents for the first full review in May. Unlike an expedited review, a full review is reviewed by all the IRB committee members and therefore a review meeting is scheduled once or twice a month. There is a submission deadline approximately two weeks before a meeting date and if you miss the deadline, you might have to wait another month. After going through numerous emails with my professor and people from IRB, long story short, we obtained the protocol approval on July 11 (which happened to be my birthday) after two full-reviews in total.
So now what?
Obtaining the protocol approval from UIC does not let us start the research right away. To obtain the final IRB approval, I must submit an IRB-equivalent approval from the local research institute (Share India) and all the research instruments translated in local languages to the IRB committee at UIC. One must be aware that any kind of unexpected change in plans tends to accompany with international research. The Share India researcher who is in our research team submitted their IRB application in June and an IRB review by the director of Share India was expected to happen in early July. However, the meeting had been postponed multiple times for unknown reasons and as of July 29, we are still waiting for the IRB-equivalent approval from Share India. As my return date (early August) is approaching, we are trying to do our best to coordinate with the local researchers and make sure everything is in place so that the research can move along smoothly once the approval is obtained after I leave India. We piloted the questionnaire a few times with my translator who will perform interviews even after I leave and make sure together every step of the research procedures. I discussed with the local researchers and the host organization on how to handle money for honorarium given to research subjects and made sure everyone on the team is on the same page.
Important Lessons
What are the lessons I’ve learned from this when performing international research?:
1). Prepare multiple backup plans. Not just plan B but also plan C, D, E, F…. etc., because there are things you simply have no control over and you have to be flexible.
2). Even when things did not go as planned, you still have many things you can do to help your research improve.
3). Pilot a data collection process first and ideally do so in an environment as close to the actual setting as possible. There is always something you wouldn’t know or notice when you were planning it on papers.
4). If a translation is involved, talk with a translator and make sure you and the translator interpret sentences in the same way. Particularly, double-check any double-negative sentences because misinterpretation can yield a completely opposite outcome.
5). Most importantly, don’t upset yourself too much with unexpected turns of events. Be calm and realistically optimistic. Making myself busy with extra work from 2) helped me stay calm and productive.
Despite that it is likely that I will not be able to attend the data collection phase, this journey from research planning has offered me many learning opportunities to grow as a public health student, a researcher and as a person. And of course, data collection is just one phase of this entire research process. We will still have to do data analysis and interpretation of the results, which will be a great exercise of real-life application of epidemiological/statistical knowledge as an Epidemiology student.
Mayuko's Blog Post

Food Insecurity and Diet
My previous post mentioned the adherence to antiretroviral therapy (ART) and ART center. In this post, I would like to focus on another main theme of our research, food insecurity. Food insecurity refers to a lack of physical, social and economic access to sufficient, safe and nutritious food to meet dietary needs. But before jumping into food insecurity among female sex workers (FSWs), there are a few things I noticed about diet and lifestyle of the locals these past 6 weeks. First, as you may imagine, if you know India is a religious country, there are a great number of vegetarians/vegans here. Hindu and Islam prohibit the consumption of beef and pork respectively. But the religions are not the only reasons why people eat less meat or no meat at all. Meat, regardless of what type it is, is much more expensive than beans and vegetables. Although animal products are relatively more expensive than vegetables and beans also in the United States, the price disparity seems much larger in India. There even seems to be a general notion that meat, particularly chicken or mutton, is prepared and enjoyed rather on a somewhat special occasion: paycheck day, birthday, anniversary etc. In the past month, I have been eating vegetable or bean curry most of the time and occasionally when chicken curry is served on someone’s birthday, I secretly high-five myself. I guess I was a little unprepared for the vegetarian life.
If chicken is considered expensive among the ordinary locals, what can the poor, who are more likely to experience food insecurity, afford? I heard at my host NGO that the poor fill themselves up with rice, flour and cheap vegetables like potatoes (all carbs basically). Beans are the most affordable source of protein but rice is cheaper. As an inevitable consequence, they will develop diabetes in later life due to the chronic overload of carbs.
.

Nutritional Support Programs for the Poor and FSWs
In Hyderabad, some NGOs and temples offer free nutritional support to the poor and the socially vulnerable who suffer from food insecurity, including FSWs. Last week I visited the Gandhi Hospital again. This time, the visit was a part of my fieldwork to learn more about nutritional support available to FSWs in Hyderabad. Knowing whether any free nutritional support by NGO, governments or religious institutions is available to these women and if so, what kind of nutritional support and how often it is available should be informative for our research about food insecurity. People at the ART center remembered my face from my previous visit and they helped me identify some NGO and government programs of nutritional support to the poor and possibly people living with HIV. Coincidently, on my way back from the Gandhi Hospital, I encountered the scene of free lunch distribution to the poor by this NGO, Sani Welfare Foundation, on a street next to the hospital. I almost felt it was meant to be because I just saw an online news article about the NGO’s contribution to the poor in Hyderabad. Although there are a few NGO programs and government-run food rationing for the economically disadvantaged, to the best of my knowledge, currently there is no free nutritional support program in Hyderabad specifically targeting FSWs. FSWs could possibly access some of the free meals for the economically disadvantaged since FSWs are also the economically disadvantaged ones.
.

Nutritional Meal Packages
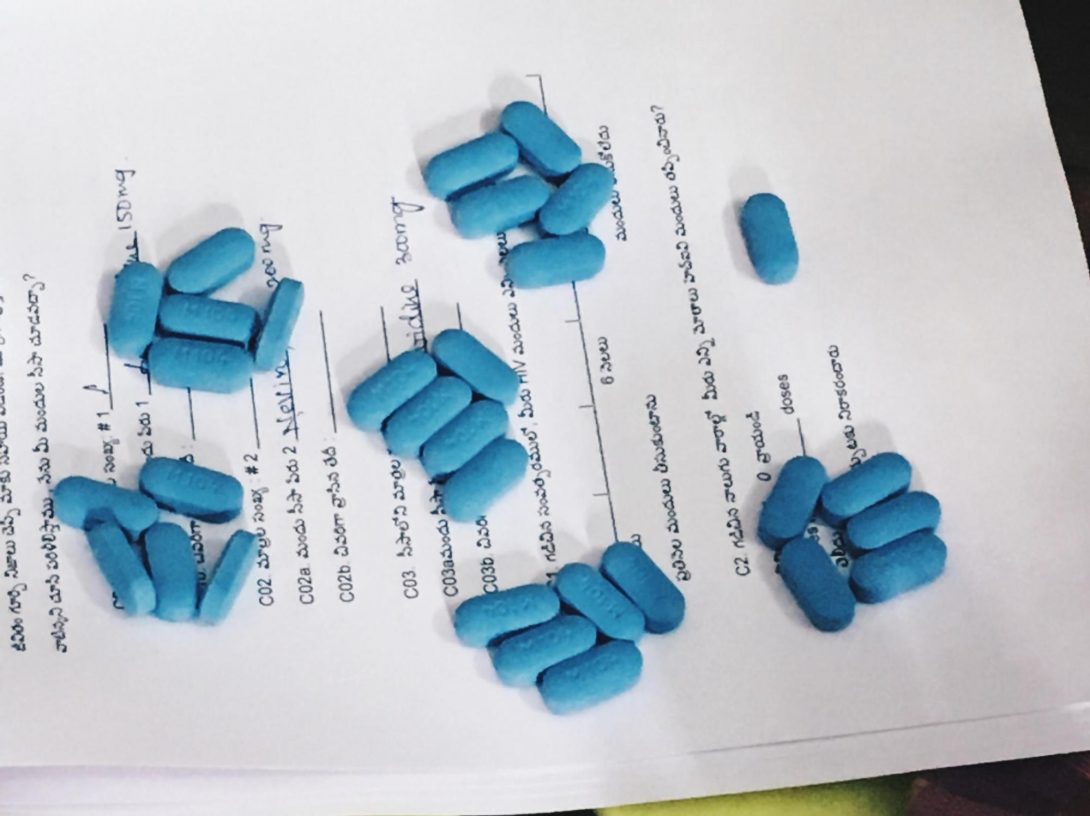
In my first few weeks when I didn’t feel well (possibly my body was adjusting to the new environment), CMM (the host organization) served me curry and rice cooked from a meal package distributed to the FSWs as nutritional support at CMM. This meal package is provided by Stop Hunger Now in India and sponsored by Google India. It contains fortified rice and legumes with a vitamin supplement. CMM receive boxes of these meal packages every year but these packages are packed only once a year. More of sustainable nutritional support that can supplement with a good source of protein, minerals, and vitamins for these women is much needed now. Our questionnaire-based research will hopefully provide deeper insights into the issues around food insecurity among FSWs and lead to future interventions.
.
The nutritional meal package by the Stop Hunger Now in India. One package can serve 6 meals.
Mayuko's Blog Post

ART Adherence
This post might be a little boring for some readers because it’s about a very specific public health topic of HIV/AIDS and medical adherence. What’s medical adherence? Medical adherence refers to adhering to medicine as prescribed by physicians. In the public health perspective, medical adherence has been an emerging challenge for infectious diseases like HIV/AIDS. There are many government/NGO programs that facilitate free provision of medicines but, with a lack of medical adherence, diseases that can be treated or prevented with today’s medicine might not be treated or prevented. This will be extremely inefficient and costly for the government, NGOs and the society. This is one of the reasons why our research focuses on medical adherence among HIV-patients, for better HIV/AIDS control in India.
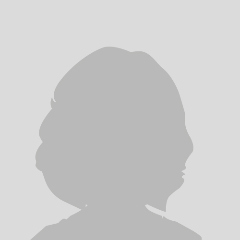
Antiretroviral Therapy (ART) Center
I visited an ART center at the Gandhi Hospital in Hyderabad with my translator from Share India the other day. The ART center is where people living with HIV come every month to pick up their prescribed pills of antiretroviral therapy (ART) and there are 28 ART centers in Hyderabad as of today (July 2017). The purpose of the visit was to learn what the experience of ART collection would be like for people living with HIV. (side note: our research is a cross-sectional questionnaire-based research on the factors associated with adherence to ART among female sex workers living with HIV.) The field work inquiry like this should be informative and helpful to understand further how ART collection process could potentially influence on medical adherence, such as experiences of commuting, waiting time, interactions with hospital staffs, ART counseling, ART stock availability etc.
The Indian government has provided free ART to people living with HIV and government hospitals are the major places for them to pick up their ART medicine regularly. When we visited the ART center at the hospital on the weekday morning, the rooms and hallway were packed with people. Although I could not document the hospital visit in photos because it would require special permission in advance, the information obtained on the day offered me deeper insights into things like the waiting time for ART collection, the process one would go through for ART pick up, availability of ART stocks and interactions with doctors and adherence counselors.
For example, two random patients who were waiting in the line for ART collection told me via my translator that they wait for about 40-50 minutes usually and the longest they have waited for was 2-3 hours. The long waiting time is a daunting experience for most of the people and can be discouraging to commute and collect ART every month for some patients. I also noticed that interactions with doctors and ART adherence counselors seem to be quick and nothing more than minimal. Although this might be inevitable since there were long lines, solely from the perspective of ART adherence, it would be helpful if doctors and counselors would take more time to ask each patient who missed doses why he/she missed and give some advice on how to prevent missing doses. Later, I also had a chance to talk with a doctor and an ART adherence counselor in person and they gave me first-hand observations and experiences they had with HIV patients at the ART collection center.
Overall, it was a very educational visit and I think it did prepare me a little for up-coming interview sessions with female sex workers living with HIV in the research after having a glimpse of their common experience at an ART collection center.
Mayuko's Blog Post

I joined another casual meeting with peer educators and outreach workers the other day when the host organization, CMM, organized it upon my UIC supervisor’s arrival. We had a translator next to us who interpreted what these women said to us. This time we talked about barriers to adherence to antiretroviral therapy (ART) among female sex workers (FSWs) living with HIV, which is our main focus in the research we are conducting here. Adherence to ART is one of the focal points in a successful HIV treatment regime. Without adherence to ART, HIV virus won’t be suppressed efficiently and a patient will be more prone to opportunistic infections such as TB, pneumonia, and cancer as immunity (# of CD4 T cells) goes down. Non-adherence to ART also allows the HIV virus to develop and spread to others. For these reasons, free provision of ART alone is not enough but rather adherence to ART is the key in efficient HIV control.
Stigma
The first topic we talked about was stigma. Do FSWs experience stigma and prejudices for being a sex worker living with HIV? If so, does this affect their ability to adhere to ART? The answers from the peer educators and outreach workers were “yes”. For a long time, FSWs have been socially looked down upon as uneducated, promiscuous women who earn money by selling their bodies with their own will. The truth is, as I wrote in my previous posts, the majority of FSWs are forced into sex work due to either sex trafficking or out of extreme poverty. Negative media coverages on FSWs have reinforced such false presumption for a long time, which is recently starting to change. A newspaper reporter even came to CMM and interviewed the FSWs to hear out their real voices.
Nonetheless, it will take a while to change societal perception on FSWs. The peer educators said one of the major reasons why FSWs miss their doses of ART is that they fear customers may see a pill bottle and therefore can’t bring the pill bottle to their work. If customers see an ART pill bottle and discover HIV status of an FSW, she may lose the customers and it will lead to potential abuse by pimps and impact on her living.
Police Violence
Police violence and arresting are another reason why FSWs prefer not to bring a pill bottle with them to their work. Sex work is illegal in India and FSWs are the target of arrest. When police find a target, police scrutinize her belongings (bag, cell phone etc.) to see if she is a sex worker or not. Having condoms, an ART pill bottle or drug in her bag would be interpreted as evidence of engagement in sex work. One of the outreach workers told us that police get promoted when they achieve a certain number of FSW to arrest. Therefore, FSWs don’t want to bring their pill bottle to their work in case of a potential encounter with police. When FSWs are arrested, they would not have access to their ART at a jail, which leads to missing doses of ART. Arresting can span a week or even a few months.
Food insecurity
Food insecurity is also a common barrier to adherence to ART among FSWs in India. To avoid side effects including dizziness and upset stomach, HIV patients are recommended to take ART pills with food. When FSWs are deprived of food, they don’t like to take ART pills because of the side effects. Experiences of food insecurity are often linked with poverty and single parenting, which is also commonly experienced by FSWs.
Hearing out the people who have seen the life of FSWs in person was very informative. When you are in the United States, it is very difficult to collect real voices from these women in India without the help of the local NGO because a) you are considered as an outsider, b) language barrier and c) voices from socially vulnerable groups like FSWs are rarely heard in public. Today’s technologically advanced society might give us some illusions that we can get almost anything and any information from anywhere in the world via information/communication technology like the Internet, Skype, social media and other online services. Yet, there is always something that we wouldn’t know until we actually go out, meet people and hear their real voices. Furthermore, such information obtained in person is often more valuable than information you could find with a few clicks on the Internet at your home. Some street-based FSWs that CMM is in touch with don’t even own a cell phone. Without the field work of the peer educators and outreach workers who physically visit each FSW on streets, we would not know about the life of these FSWs. In this regard, this was a great session.
Mayuko's Blog Post
The Institutional Review Board (IRB) process is like running a marathon, or at least for me as a first timer going through this it is. Since our second submission of modifications that we filed before my arrival in India, I was waiting for a protocol approval from the IRB committee at UIC so that we can start our research. I’m not going to lie, the waiting time had kept me being a little nervous as my time in India had passed by. In addition, I had some dizziness from the recent diet shift to vegetarian curry in the past few weeks in India. Hence, on the morning of July 11, which was my birthday, I was not feeling great physically and mentally. But it turned out to be a day filled with a miracle and surprises…
The Email About The IRB Approval
The morning started off with a birthday miracle, as I call it. I woke up and found delightful news in my UIC email inbox. My UIC supervisor forwarded me the email with attachments titled
‘Approval Notice- Initial Review (Response to Deferral)’.
Just to be sure, I had to read the attached report a few times to believe this is really about the protocol approval by the IRB committee. Hallelujah! After three months since our first submission to the IRB review in April, we finally obtained the protocol approval. With the time spent on preparation for necessary documents considered, it has been more than six months since we have worked on IRB submission. Even without the IRB approval, I would have continued making my stay in India as fruitful and meaningful as possible. However, my main purpose of my stay in India is to perform the questionnaire on 70 female sex workers living with HIV in Hyderabad. The delightful news that we can finally start our research, instantly blew my anxiety away.
More surprises to come
The IRB approval was not the only thing that made my birthday as special as it could be. People at my host organization, Chaithanya Mahila Mandali (CMM) organized a birthday cake ceremony for me as it is their tradition. A few hours before the cake ceremony, they told me that they will take me out to “somewhere.” We got in a car and it turned out we were heading to a small department store in the downtown Hyderabad. As a very thoughtful and generous gesture of them, they said they will buy me a traditional Indian dress as a birthday gift so that I can wear it for the cake ceremony! As Indian tradition, a girl wears a traditional dress on her birthday. This explains why some girls at the Children Home asked me the day before what I would be wearing on my birthday. The girls looked confused and even a little shocked when I smiled and said I don’t have any specific plan on my outfit yet.
Among hundreds of colorful traditional dresses with different patterns and designs, we picked a two-piece dress that comes with a silky green top with gold beads embroidered and a long flair rouge skirt with leaf patterns in gold. The vibrant colors of silky green and gold-rouge complimented my medium skin complexion. Also, a two-piece dress was perfect for me as the length is adjustable based on my petite height.
In addition to the dress, they spoiled me with kulfi too. Kulfi is a traditional Indian ice cream made from milk alone and often topped with spices and nuts. They treated me to Kulfi at the kulfi vendor in front of the store. I instantly loved kulfi! It is not as heavy or greasy as Western ice cream and I can taste the rich flavor of milk with some hint of exotic spices and crunchy nuts on the surface.
.

Birthday cake ceremony and Chicken Feast
The birthday cake ceremony along with gifts of birthday songs from the 45 children made me feel welcomed to this big family. The older girls played a guitar, xylophone and digital piano. I exchanged a bite of the cake with everyone and received heart-melting birthday cards from the children.
In return, I sponsored the special chicken dinner for everyone as a surprise. The cooking auntie prepared a delicious chicken curry for 50 people (45 children 5 adults) with the 15kg of chicken I bought earlier. For many locals whose daily meals are vegetarian curry with rice or chapatti (flatbread), chicken is eaten only on a special occasion because it is not cheap in India. As a non-vegetarian person, I’ve personally been thinking the children should eat more meats for their muscle development. And after all, these children said they love chicken and they don’t get to eat it very often. Seeing the children enjoying the chicken curry made me happy.
Starting with the news of the IRB approval and ending with the birthday cake ceremony and chicken feast, my birthday was filled with heartwarming surprises thanks to everyone at CMM. I truly appreciate their thoughtful gesture on not making me feel like a stranger on my birthday and on welcoming me as a part of their family.
.

The birthday cake ceremony at the CMM. The founder and mother figure of the CMM (left) and I (right) in the traditional Indian dress. *Photo credit: the project manager at the CMM.
.

*The contents of this blog do not represent any position of the School of Public Health but are mine personally. All the photos used are taken by me, unless a photo credit is mentioned.
Mayuko's Blog Post

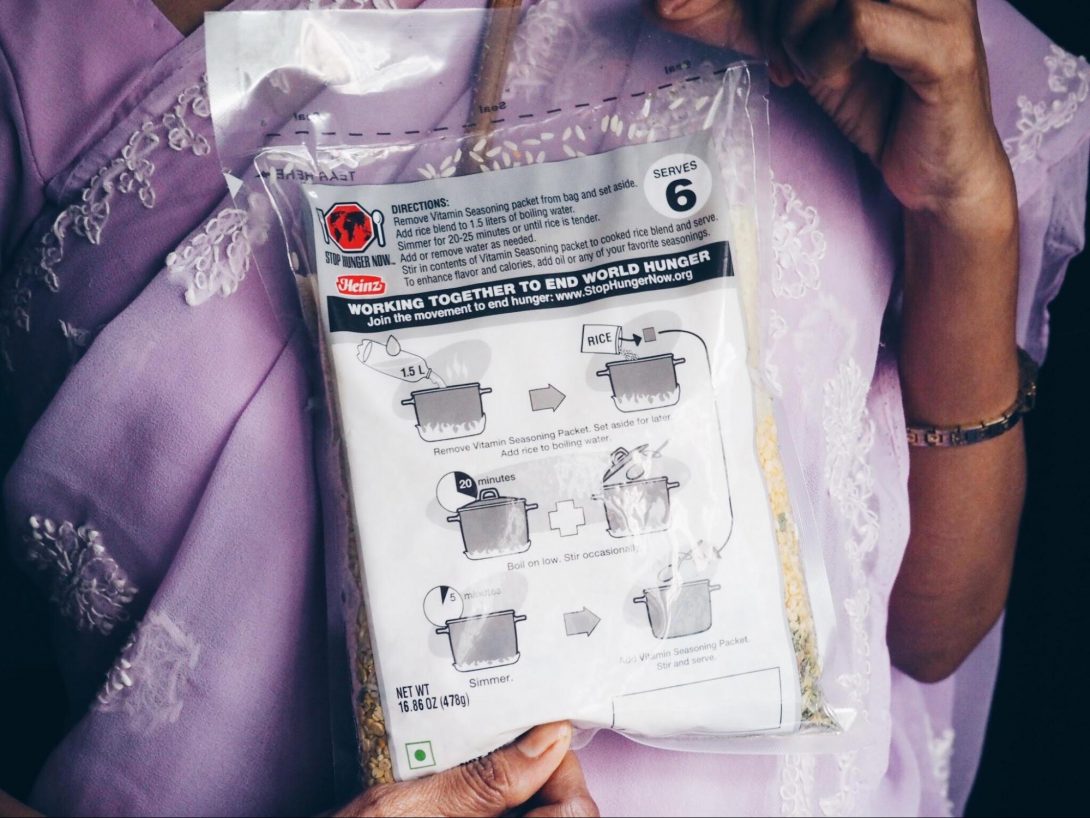
Basic School Supplies for Children
I joined people from my host organization for a day trip to public schools in rural areas of Hyderabad. The goal of the day is to deliver and donate school supplies to children at three public schools in neglected rural areas where often government support is scarce. This is a part of the new project Chaithanya Mahila Mandali (CMM) has recently launched. CMM had collected notebooks, backpacks, pencils, erasers and pencil cases from donors in the past months. We packed all the school supplies (enough to provide for more than 850 students) into a van in an assembly-line way and departed for the day trip. After driving through busy downtown Hyderabad for one and a half hours and getting off the highway, it suddenly revealed peaceful bucolic landscapes with water buffalos and farmers on rice fields. No air pollution, no honking sounds, and much fewer people. It was nice and far from the most common image people or at least I would have for India (now I really wish that I took a photo).
For another half an hour or so driving along the rice fields and vegetable farms, we reached the first village we planned to drop by. The school was located near the entrance of the village. We got out of the van and started to hand out a set of notebooks, pencils, erasers, a pencil case and a backpack to each child from grade one to grade ten (In India, grade eleven and twelve are affiliated with a college). The children were very curious about me, probably because they don’t have much exposure to a foreigner. Just like the children at the CMM’s Children Home, they asked all possible questions at about my name, where I am from, my birthday, whether I like India, my siblings, even my mother’s name and birthday. Two ears are not enough when you are around Indian kids! After we had some fun times and took photos together, we moved to different villages for two other schools and handed out the remaining school supplies.
.
Reality of Public Schools in Rural Areas
What do all three schools have in common? First, they are all in poor and neglected rural areas where not even single bus routes are installed and the schools are the only school in each village. Second, they are public schools, which means the government covers tuition from grade one to grade six and free lunch is served for all children. Third, most of the villagers are farmers or shepherds if they have a job. Summing all of this up, these commonalities mean that the children walk for a few hours to school and they come to school just to have free lunch. After grade six when tuition is not free anymore, many of them start to work for farm work or something else and are encouraged to marry before twenty.
Children need to come to school to receive an education. As it sounds almost cliché, education plays pivotal roles in increasing chances to move up the social and economic ladder. However, when financially challenged, education is often difficult to be prioritized. That’s why the organization like CMM delivers basic school supplies to these children and help to provide them the suitable environment for learning.
.

Homecoming
Apparently, one of the children at the Children’s Home arrived a year ago, from the most remote village we visited. She came with us for this trip to the rural village for a homecoming reunion with her relatives and friends who still live there. She lived there until the age of 13 and she moved to the Children’s Home with her younger sister when she lost her parents and no relatives were able to support them financially. Her mother was domestically abused by her father and she committed suicide. Her father also threw himself in a well, fearing her mother’s suicide would ruin his reputation at the village. Such dark past of her family was almost unimaginable from her carefree personality and the peaceful village landscape. In the reunion with her old friends and relatives, she was weeping with joy for reunion and sorrow for separation. Despite my eager attempt, I would never be able to fully understand how it feels to go through the loss of parents at a young age and becoming an orphan with a younger sibling. I can only wish that their lives will be filled with more happiness and blessings than the sorrow and pain they’ve experienced in their early life.
.

A small community in the countryside. No bus route is installed. If one goes to the city of Hyderabad, he takes either an auto- rickshaw (a small taxi) or walks.
.

Poor and neglected but beautiful and peaceful villages in rural areas. An old woman is plucking henna leaves. Henna leaves are used for traditional henna tattoo on hands and hair dye among women.
Mayuko's Blog Post

Leprosy and Sivananda Rehabilitation Home
I had an opportunity to visit the Sivananda Rehabilitation Home in my second week. Sivananda Rehabilitation Home has served for leprosy (Hansen’s disease) patients by providing medical treatments and rehabilitation support since 1958. The day trip to the leprosy center was interesting to me because HIV/AIDS and leprosy have at least three things in common:
1. Being an infectious disease and being highly stigmatized by the society for a long time
2. Infected individuals can still live a long healthy life due to the medical advancements we have embraced today
a. Leprosy is curable with multidrug therapy and HIV virus is not 100% curable yet but can be under control with full adherence to antiretroviral therapy (ART).
3. India is a country with the third largest HIV/AIDS epidemic and the highest leprosy incidence in the world
As an MPH student, I felt lucky to sneak-peak the two major public health challenges of this country at the same time.
Leprosy has been documented since the early history of human in many parts of the world. With manifestation of crooked fingers, deformation of skin and damage on nerves, leprosy patients have been feared and stigmatized as “a sinner” and “curse or punishment from God” for centuries. They were shunned from the society and forced to isolate themselves in an island to form its own community. Until the Norwegian doctor, Gerhard Hansen identified that leprosy is caused by the germ, people had believed leprosy was hereditary and pregnant women with leprosy had been the target for compulsory sterilization and abortion as a part of the eugenics program. With today’s medical knowledge, leprosy is recognized as one of the least infectious diseases for which 95 percent of the population have natural immunity and multidrug therapy is the effective treatment for the infection.
.

The tour at the rehabilitation home
One of the physiotherapists showed us around the rehabilitation home. While touring different parts of the facility, he introduced us some of the patients in progress of rehabilitation. One man showed us his crooked fingers and damaged foot in a cobbler, which are the typical manifestations of leprosy. The physiotherapist explained that at the rehabilitation home, a patient with crooked fingers and damaged feet take physiotherapy to practice stretching out their fingers and walking in cobblers and a patient with nose disfigurement can take a reconstructive surgery.
But what inspired me the most was the importance of counseling for effective rehabilitation. With low self-esteem and loss of dignity over the course of experiencing stigma and prejudice, some leprosy patients have given up on attempts to treat the disease and rehabilitate themselves in the beginning. For that reason, a physiotherapist often starts off with counseling care to promote positive frame of mind so that patients can believe in positive impacts of rehabilitation.
I also liked their mission to promote Integration, Dignity and Economic Advancement (IDEA) for leprosy patients. At the rehabilitation home, people who were once leprosy patients themselves are now working at the rehabilitation home and taking care of other leprosy patients. Not only do they take care of leprosy patients as peer staffs who share similar experiences but they also regain their dignity and self-confidence in their own abilities through experiences of serving others. The rehabilitation home also offers vocational training where leprosy patients can learn how to weave textiles and construct cobblers and wheelchairs to encourage economic advancement.
The field trip to the Sivananda Rehabilitation Home was very interesting overall. As both leprosy and HIV/AIDS are highly stigmatized diseases, I definitely can see some of the approaches to leprosy rehabilitation (i.e counseling to the positive frame of mind, IDEA) are also quite applicable to HIV/AIDS treatments. Special thanks to the Sivananda Rehabilitation Home who showed us around!
.

The woman showed us a room for cobbler making.
.

*The contents of this blog do not represent any position of the School of Public Health but are mine personally. All the photos used are taken by me.
Mayuko's Blog Post

Prostitution and Sex Slavery in India
In India, prostitution is illegal and socially looked down upon. The Indian traditional society perceives breaking abstinence as a huge taboo for youths before marriage for religious and cultural reasons. This may partially explain why engagement in sex work is severely disdained with the false presumption that all the female sex workers voluntarily choose to be promiscuous and earn money from sex work.
The project manager at CMM however, told me that only a fraction of a percent of female sex workers is voluntary. Voluntary sex workers, although they are very few, include housewives, college girls and nameless actresses who would have other means to financially support themselves and their families but choose to take clients out of boredom or in need of quick cash. According to him, unfortunately, the majority are sex-trafficked women who are trapped and forced by their brokers/pimps at brothels, or have no other means to financially support themselves and their families out of poverty (60 percent for the former and 30 percent for the latter based on his statistics). Brokers at brothels speak to girls from poor families that they will be introduced to a well-paid job so that the girls can support their family and this turns out to be prostitution. Or, they are human-trafficked for sex slavery. By the time girls try to escape, brokers force them to stay. Even if she is lucky enough to escape and go back to her community, she is likely to return to prostitution due to experiences of stigma and rejection from her family and community.
The rest of less than 10 percent are in a completely distinct category of traditional prostitution called the Devadasi System practiced mainly in South India. The Devadasi System has justified temple prostitution in the name of God for centuries. Young girls from the lower caste are dedicated to appeasing gods and goddesses by remaining as a sexual servant for the priest and upper-caste men for the rest of their lives. I was completely ignorant about this traditionally-imposed form of prostitution until Mr. Jaya explained it to me.
Getting back to the initial topic, the majority of women in poverty who are forced into sex slavery suffer from the burden of false presumption by the society that these women voluntarily choose to be sex workers. Stigma, neglect, police violence, negative media coverage and a lack of general understanding of these women’s struggles often accompany with such societal presumption. CMM reaches out to empower the neglected, highly stigmatized group of women in Hyderabad with help of outreach workers and peer educators.
Discussion with peer educators and outreach workers
One afternoon, CMM organized a causal meeting with peer educators and outreach workers for me. Outreach workers coordinate counseling appointments and regular follow-up calls or visits. They are literate women who were once sex workers but now work at CMM full-time. On the other hands, peer educators are women who are sex workers at present and work for CMM on a part-time basis. They have the most proximate contacts with other sex workers and act as a peer/mentor in educating female sex workers. Peer educators work for the NGO without their broker/employers/pimp’s knowing. In other words, they are the real insiders to know about and contact female sex workers in Hyderabad. Without these peer educators and outreach workers who know female sex workers well, female sex workers are difficult to reach for NGOs and researchers. In the meeting, these women explained to me about the importance of their work and how they are implementing services and care on female sex workers in the field.
.

STIs and HIV/AIDS Education
Female sex workers are extremely vulnerable to STIs and HIV/AIDS. Peer educators showed me picture books they use to educate female sex workers about risky sexual behaviors and the importance of the use of condoms to prevent STIs and HIV/AIDS infections. Furthermore, they also teach more technical tips on how to convince their clients to use condoms (ex. how to flow convincing conversations). In convincing clients for safe sexual practices, they advise explaining to clients with “this will protect not only me but also you, your wife and children.” To my surprise, some clients not only agree with using a condom but also thank the female sex worker for teaching an important lesson. But of course, others remain hesitant. In case clients still disagree, women learn how to secretly make him wear a condom too (ex. Hiding a condom in her mouth and apply it during oral sex before insertive intercourse).
.
Counseling Services for addiction and behavioral change promotion
Counseling services play vital roles in psycho-social support for female sex workers and women who used to be female sex workers. Depression, Post-Traumatic Stress Disorder and substance/alcohol addiction are not so uncommon among women suffering from the emotional trauma of sex-trafficking. Peer educators and outreach workers help these women with overcoming trauma and addiction through regular follow-ups and friendly contacts. In addition to the experiences of forced sex work, a discovery of HIV-positive status can double the emotional burden on these women, as being HIV/AIDS- positive is as highly-stigmatized as being sex workers. Educating these women about HIV/AIDS and the importance of medical adherence to antiretroviral therapy (ART; HIV/AIDS medicines) is another essential aspect of the counseling services. Non-adherence to ART not only exacerbates women’s health but also leads to developing resistant HIV virus and its transmission to others.
One of the peer educators told me that there was an HIV-positive woman who answered in the initial stage of counseling sessions that she preferred NOT to use condoms so that she can infect their clients with HIV as revenge. It may sound corrupted to us but I imagine it would be an inevitable mindset resulting from repeated denials of self-dignity over the course of forced sex work and abuse. Changing slowly this kind of negative mindset with traumatic experiences into the positive one is also one of the important jobs for peer educators and outreach workers.
Protect Women from HIV and Bring Positive Impacts for All
Lastly, the project manager explained to me why what they are doing is very important and why they focus on female sex workers for HIV/AIDS prevention. If they provide female sex workers education and resources to protect themselves from HIV/AIDS, these women can prevent HIV transmission to their clients and even teach their clients why this is important, which eventually turns out to protect wives and children of the clients and everyone else in the community. Targeting male clients in prevention control is rather difficult because they come from anywhere and have no specific common profiles; while targeting female sex workers is different because we know they are often connected to their network and work in certain neighborhoods. Overall it was a very informative talk. It gave me much more insight into the work of peer educators and outreach workers as well as the struggles of female sex workers that I was not aware of.
*The contents of this blog do not represent any position of the School of Public Health but are mine personally. All the photos used are taken by me.
Mayuko's Blog Post
As briefly mentioned in my previous post, CMM, the host organization that I am working with, is a NGO that strives to empower girls and women vulnerable to sex slavery in Hyderabad. They outreach, educate and offer various forms of support and resources to female sex workers. However, CMM’s contribution to the community is not limited to care for female sex workers. CMM also serves as a home for 44 children of the sex-trafficked victims. These children are not only safe from risks of entry to sex slavery but also receiving educational, social and nutritional support. These children either lost their mothers (i.e they passed away due to HIV/AIDS and other diseases) or, they are alive but can’t fully take care of their children (i.e poverty, addiction or neglect). At CMM, the children eat, study, play and sleep together as one big family with on-site caregiving staffs.
Education as a tool to break the poverty cycle
As we all know, education is a powerful tool to break the poverty cycle. Particularly, education for children is essential to help new generations with getting out of poverty and stop the poverty in the families/communities.
The project manager at CMM, told me the endless cycle of sex slavery in India. Often, girls from poor families are tricked into sex slavery believing they would be introduced to well-paid jobs so that they can support their family. By the time the girls realize they are forced to sex slavery, they cannot run away easily or even if they can, they choose to come back to the sex work industry due to stigmatization and rejection by their own families and relatives. In India, sex before marriage is a huge taboo for religious and cultural reasons, let alone engagement in sex work. Sex workers are looked down upon with disgrace and shame by the society and treated as lower than the lowest caste. Sex workers’ daughters also follow the same path to sex work as their mothers at early age instead of going to school. Seeing their mothers in sex work in everyday life, sex slavery is so normalized to eyes of the daughters that children bring customers to their mother for sex work. This cycle of sex slavery continues to the next generation. Therefore, protecting children from sex slavery and giving them proper mainstream education are very important to break the cycle of sex slavery and poverty.
At CMM, caregivers help children with catching up with mainstream education. CMM also focuses on English and computer education from early stages of child development so that children will be more employable and able to stand on their own feet in the future. Children learn speaking and writing both in Telugu and English. At the IT center where six computers are installed, children learn basic computer skills such as Microsoft Office software and beyond with help of volunteers. The IT center was set up recently thanks to the donation from ACASS Canada, the Montreal-based business aviation company. It is truly wonderful to see these children at the orphanage are given opportunities, like other children, to learn the global language and computers.
Celebrating every child’s birthdays for a happy long life ahead
On my third day in India, one of the girls at CMM had her eighth birthday. At CMM, every child’s birthday is celebrated with a birthday cake and a gift of birthday song from other children. After dinner, children gathered at the main room and sat in front of the table with a birthday cake. The birthday girl of the day, stood in front of the birthday cake table and the children started to sing the birthday song.
“Happy birthday to you happy birthday to you
happy birthday dear Subratika happy birthday to you!
(2nd verse) Happy blessing to you happy blessing to you
happy blessing dear Subratika happy blessing to you!
(3rd verse) Happy long life to you happy long life to you!
Happy long life dear Subratika happy long life to you!”
When I heard the third verse of the song which I’ve never heard in the US, I realized that they really meant it. Birthday is not just a day you can eat cakes, get gifts or party with friends and family but it truly is an anniversary to appreciate your making it to a certain age and bless you for happiness and longevity. At the sight of the children celebrating and wishing other children a happy long life ahead, I couldn’t help but reflecting upon the reality of children in India where not every child may live a happy long life.
Although my research focus is primarily on female sex workers, I have been discovering many things from these children every day. I am so happy to have met them and to spend my six weeks with them at CMM. I am also hoping outcomes of what we are doing for the research (i.e investigating adherence to HIV medications among female sex workers) will eventually benefit these children and other members of the community.
*I hope my blog inspires some of you guys. If you feel inspired and would like to know more about these children, check it out at https://chaithanyamahilamandali.jimdo.com. You can also donate for the children and sex-trafficked victims from the link below, as CMM is in needs of funds to expand their facilities and services to more of them on streets looking for a way out of sex slavery. I created a campaign for them and I will be really grateful if you can take a look! Donation link: https://letzchange.org/campaigns/nutritional-support-for-starving-women-living-with-hivaids-mayuko-takamiya
Mayuko's Blog Post

Despite the fact that the major religion in India is Hindu, Hyderabad is an exceptional city where approximately 30-40 percent of the population are Muslim. This is due to Hyderabad’s unique historical background influenced by the Persian Empire and other neighboring Middle Eastern culture. The ancient Persian Empire (Achaemenid Empire) once had conquered the vast Eurasian continent from Turkey in the West to some parts of the current India in the East a long time ago (518 BC). Even after the rises and falls of numerous dynasties, empires and kingdoms in the region, Persian language (Farsi) remained to be the aristocratic language at Indian palaces. Particularly when the Old City of Hyderabad was the capital of the Qutb Shahi dynasty that flourished in 16th – 17thcentury, the official religion was Islam.
Today, the Old City of Hyderabad is still a Muslim-dominated area where you can find mosques, Arabic signs and Muslim women in black hijab, unlike other major cities in India. My first sightseeing in Hyderabad started in the Old City where the symbol of the city, Charminar is located. Charminar means “char=4” and “minar=minarets” in Telugu and Persian language. The symbolic four-tower monument built in 1591 is a popular tourist site in Hyderabad for being the icon of the city, cheap shopping streets and surrounding vibrant atmosphere.
.

Charminar in the front of the photo. Street vendors and restaurants surround Charminar.
.

When I visited Charminar with my colleagues, it was the early evening of June 25, which marked the end of Ramadan. Ramadan means a month of fasting and prayer and at the end of Ramadan, Muslims celebrate and greet each other saying “Eid Mubarak! (Happy blessing!)”. Charminar at the end-of-Ramadan day was packed with local people and vibrant in the celebrating mood. Trying not to lose each other in the sea of people, we walked along the pedestrian street heading to Charminar. Along the street, I saw endless street vendors selling samosas, chocolates, fruits, dried fruits, nuts, herbs, skewers, socks, trousers, shoes, sandals, spoons, towels, kitchen supplies, sunglasses, gold accessories, purses, hats for Muslims, scarves….and more. Not only they were selling pretty much ANYTHING you can think of but also at very cheap price.
.

After we reached Charminar and looked through all the vendors, we dropped by Mecca Masjid. The quad in front of the Mecca was crowded with religious people celebrating the end of Ramadan. We could go closer to the Mecca but we decided not to because it suddenly started to pour (it is rainy season from June-August in Hyderabad) and we didn’t have an umbrella with us. We gave up and waited under the entrance gate for the rain to stop. Nonetheless, it was my first time visiting a Mecca and I am glad because I wouldn’t have a chance to see it so closely when I go back to Japan (my home country) or Chicago.
After the rain became less heavy, my colleagues took us to a place near Charminar where we can have Haleem, the common dish that people eat after fasting of Ramadan. Lamb, ghee (Indian butter), dried fruits and some spices are all stewed together for 8-10 hours so that the lamb becomes tender with paste-like consistency. The look of it may not be appetizing but it was not bad at all! Haleem did remind me more of Persian/Middle Eastern stews than Indian dishes that I’ve ever tried.
.

After we ate and had some rest, we saw the main street completely soaked with the heavy rain. The street turned to be like a shallow river. I was wearing flip flops. The terrifying thought of that the rain probably washes away literally everything on the street (including feces and urine of cows and humans) and that I am walking in the sewage-laden water trembled me. But I shook myself up to keep walking. When I came back to my room later, I washed my feet and legs at least three times with body soap!
.

Despite the heavy rain and the walking in the dirty water, the visit to Charminar was so much fun. Partially because I’d neither been to an Indian street with street vendors nor experienced celebration of Ramadan. Sadly in recent years, the world has been islamophobic due to ISIS terrorisms increasingly happening almost every day. The islamophobia is often accompanied by stigma and discrimination toward innocent Muslims. Getting to know a little bit about Ramadan inspired me to learn more about what’s really about Islam, Muslims and their culture.
Mayuko's Blog Post

My first week in Hyderabad, India has almost passed. From the moment I stepped on a plane till today, it was already filled with a series of surprises and discoveries. As it is my first time visit to India, everything I see and experience appears interesting, surprising and overwhelming to me. For example, my domestic flight from Mumbai to Hyderabad was changed three times right before my departure and even changed its airline company in the last minute. My flight originally arriving in Hyderabad at 9pm turned out to arrive at 4am after ten hours layover at Mumbai airport. I felt frustrated at this unexpected change of schedule but it became a good lesson for me in the beginning of my journey to learn that things sometimes won’t go as expected in our home countries and that I need to be flexible.
After safely arriving in Hyderabad, sceneries of local people’s life that I saw the first time from the car window on the way from airport were quite interesting to me as well. As I expected from people’s stories and TV documentaries, I saw cows casually sitting on the side of streets and overwhelming number of motorcycles and auto-rickshaws with vibrant honking sounds (it was only 5am!). I was also overwhelmed at mountains of garbage that I saw here and there on the side of streets! Everything was astonishing and quite interesting to eyes of an India-newbie
So, why am I here in Hyderabad? – I am here to work on a research about adherence to antiretroviral therapy (ART) among female sex workers living with HIV under supervision of Dr. Dworkin at UIC. We will perform the questionnaire to determine factors associated with non-adherence to ART among these women in collaboration with SHARE India (local research institute) and Chaithanya Mahila Mandali (CMM). CMM is a NGO that strives to empower girls and women vulnerable to sex slavery in Hyderabad. They outreach, educate and offer various forms of support and resources to female sex workers. Through educational and social supports from CMM, girls and women learn how to protect themselves from STIs and HIV/AIDS and with getting out of the vicious cycle of sex slavery and poverty. Due to logistical reasons, the research will start in July. In the meantime, I will learn more about CMM and its roles in the community and help them with collecting funds.
.

Given wonderful opportunities to travel to India and be a part of public health research, I hope to make my six weeks as fruitful and meaningful as possible. And I am happy to document my experiences in India as a blog here on the UIC website. I will keep you updated for my next exciting six weeks! Thanks for reading!