Policy Brief: Analyzing Illinois’ Shelter-in-Place Order
Introduction
Note: this is a policy brief in a series of publications from the Social Vulnerability Group at the UIC School of Public Health's Health Policy and Administration division.
Illinois enacted Executive Orders Number 9 and 10 on Saturday, March 21 to launch telehealth reimbursement overhaul and shelter-in-place, further enhancing local state response to the COVID-19 pandemic.
Executive Order No. 9 requires telehealth services to be covered and reimbursed at the same rate as an in-person visit. This applies to all regulated Illinois insurers. For Illinoisans this includes HCSC/Blue Cross Blue Shield, Cigna and Aetna. The Order is a development of earlier telehealth service expansions in response to the COVID-19 pandemic which permitted the use of telehealth services to be delivered to any patient through commonly available technology including FaceTime, Google Hangouts or simple phone calls. This Executive Order continues to enhance Illinois’ ability to maintain social distancing for patients by exploring a novel approach to protecting providers through what we referred to earlier as “clinical distancing.”
A stay-at-home directive from the Governor’s Office was issued through COVID-19 Executive Order No. 10 on the evening of March 20th and took effect 5pm on the 21st. Previously, social distancing policies have been enacted to slow the spread of COVID-19 throughout Illinois, and this latest enactment further strengthens the State’s position on promoting policy to limit community spread. The Executive Order now mandates that everyone stays home unless absolutely necessary. The Order describes permissible travel as related to health and safety; for necessary supplies and services; outdoor activity compliant with social distancing requirements; essential work; or to take care of others. All public gatherings of any number are prohibited. Theaters, parks, country clubs and any other recreational space public or private is now closed. Cases continue to rise and increased by more than 10-fold since Illinois closed all restaurant dine-in operations. This is not totally unexpected considering what is known about the transmission and incubation period of COVID-19 paralleled with heightened local testing, but it still shows that the virus already made a considerable impact through Illinois.
Story, continued.
Stricter measures and policies are intended to stymie the spread of the pandemic, but as cases continue to rise, we will need to continue to monitor these policies’ effectiveness and the public’s compliance and willingness to adhere to them.
| MPH in Health Policy and Administration Student
Story, continued.
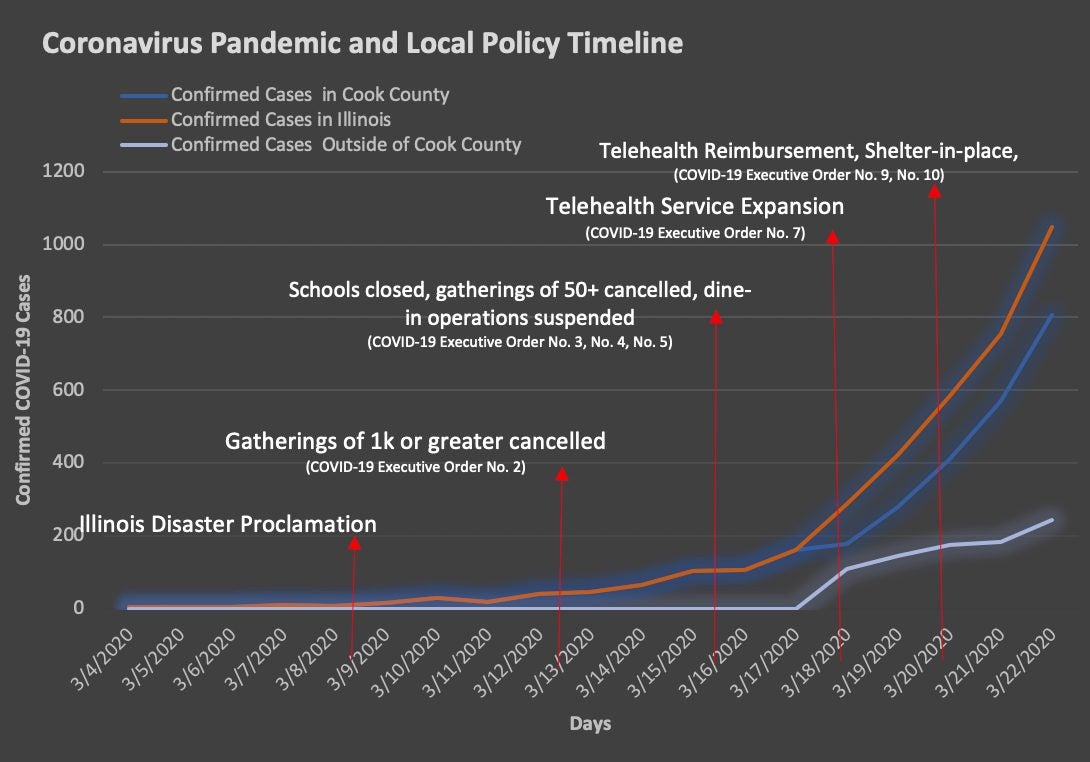
The spread of COVID-19 in Illinois is escalating, as Chicago saw 368 new confirmed cases since Friday March 19th. Illinois confirmed cases are now 1058. All five collar counties have reported confirmed COVID-19 cases and rural counites are seeing their first confirmed cases as well. Further community spread throughout Illinois can be assumed as the actual cases we estimated far exceeds the current confirmed cases (Estimating Undetected COVID-19 Cases Chicago). As the disease makes it way out of the urban and suburban counties in Illinois, to rural counties where hospital beds are fewer and the population older, telehealth services will become increasingly more vital and social distancing will continue to be paramount. Current policies in Illinois are trying to address the pandemic on multiple fronts as urban epicenters are trying to limit further community spread and rural communities will try to prevent COVID-19 from spreading if it is not already there. We will continue to track and monitor policies in detail and the impact they are having on flattening the curve of COVID-19 in Illinois.